Introduction
Understanding cholecystectomy surgical anatomy is fundamental for safe and effective gallbladder removal. Whether performing a laparoscopic or open procedure, surgeons must have precise knowledge of biliary anatomy, vascular structures, anatomical variations, and critical safety landmarks to prevent complications.
Cholecystectomy remains one of the most commonly performed abdominal surgeries worldwide, particularly for symptomatic gallstones, acute cholecystitis, biliary colic, and gallbladder polyps. Mastery of surgical anatomy directly reduces the risk of bile duct injury, bleeding, and postoperative complications.
This comprehensive guide explores cholecystectomy surgical anatomy in detail, covering anatomical landmarks, variations, vascular supply, nerve structures, and the critical view of safety (CVS) concept essential for modern surgical practice.
Overview of Cholecystectomy
A cholecystectomy is the surgical removal of the gallbladder, most commonly performed using minimally invasive techniques.
Two primary approaches include:
- Laparoscopic cholecystectomy (gold standard)
- Open cholecystectomy (used in complex or emergency cases)
Both techniques require an in-depth understanding of cholecystectomy surgical anatomy to safely identify and preserve vital structures.
Anatomy of the Gallbladder


4
The gallbladder is a pear-shaped organ located on the inferior surface of the liver in the gallbladder fossa between liver segments IVB and V.
Parts of the Gallbladder
Understanding its subdivisions is essential in cholecystectomy surgical anatomy:
- Fundus – Rounded distal portion projecting beyond the liver edge
- Body – Main central part attached to the liver bed
- Infundibulum (Hartmann’s pouch) – Dilated area near the neck
- Neck – Narrow portion that transitions into the cystic duct
The gallbladder stores and concentrates bile, releasing it through the cystic duct into the biliary tree.
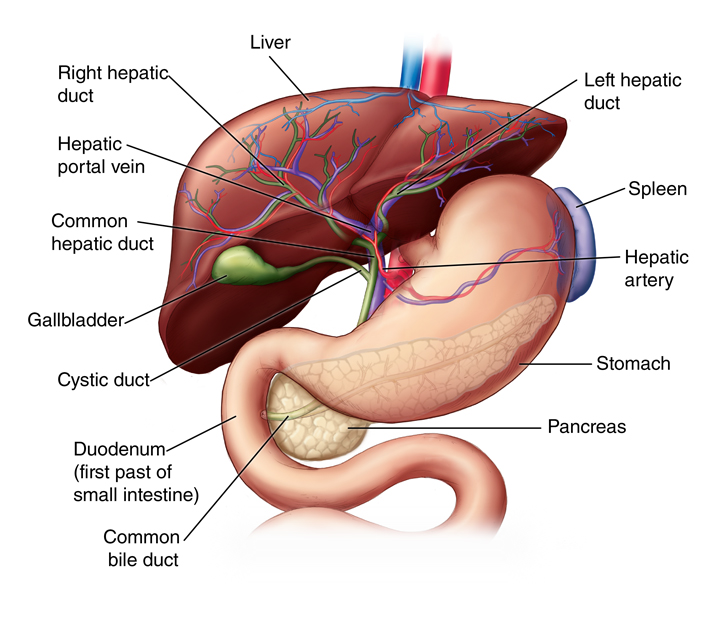
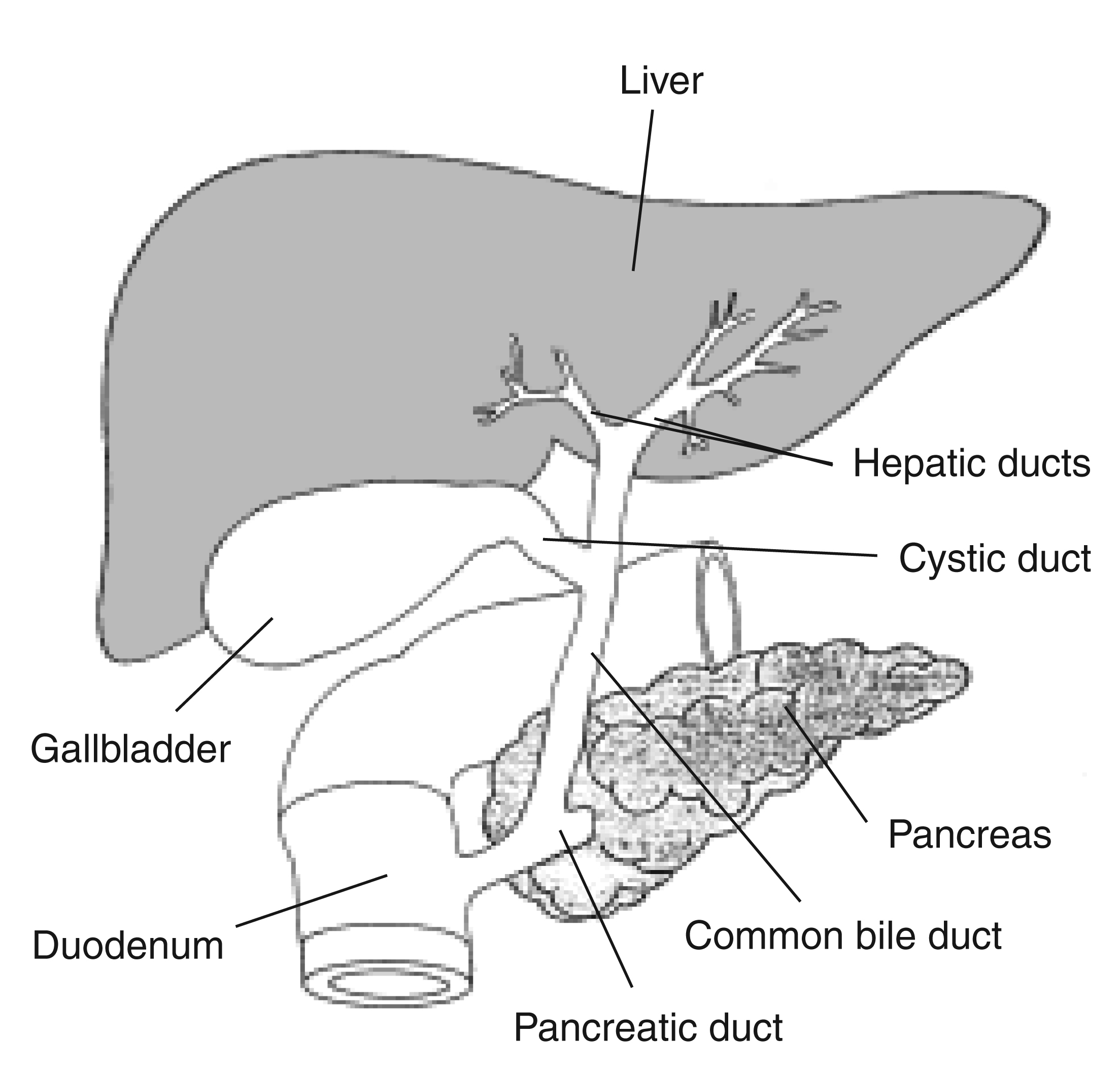
The Biliary Tree and Ductal Anatomy

4
The biliary system is central to cholecystectomy surgical anatomy.
Key Structures
- Cystic duct – Connects gallbladder to common hepatic duct
- Common hepatic duct (CHD) – Formed by right and left hepatic ducts
- Common bile duct (CBD) – Formed by union of cystic duct and CHD
Accurate identification of these structures prevents bile duct injury.
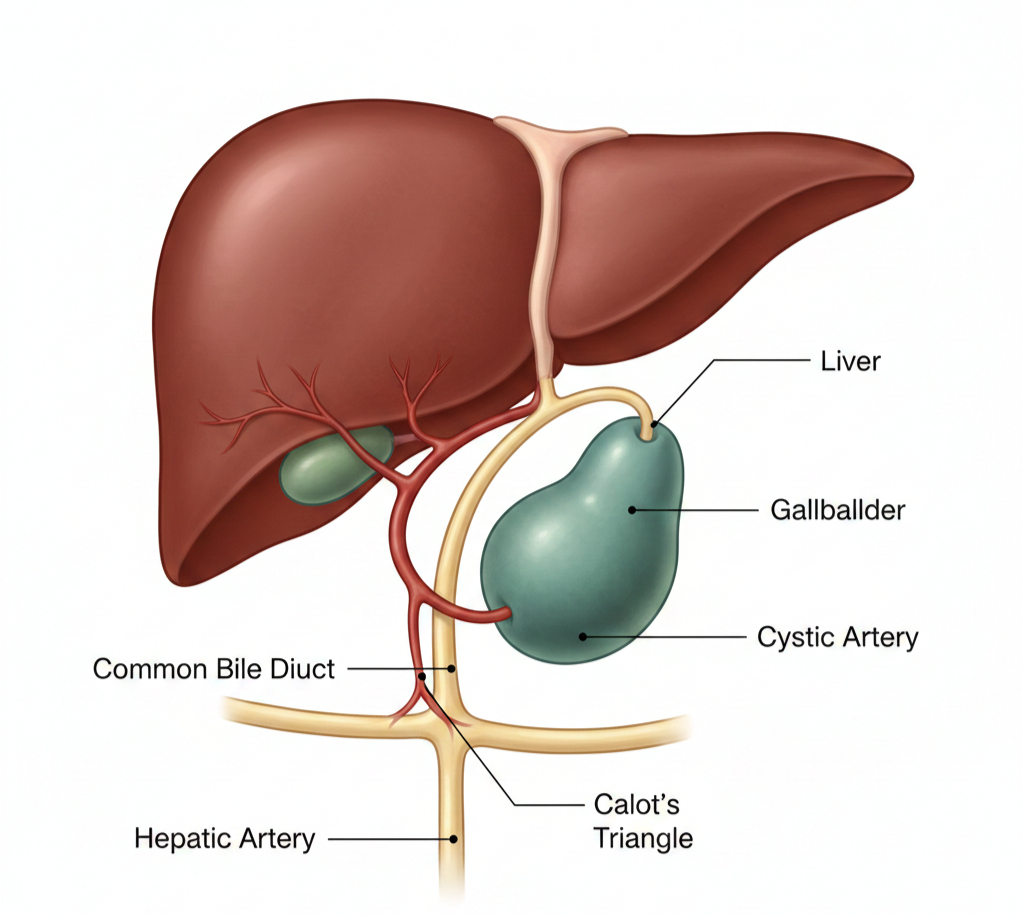
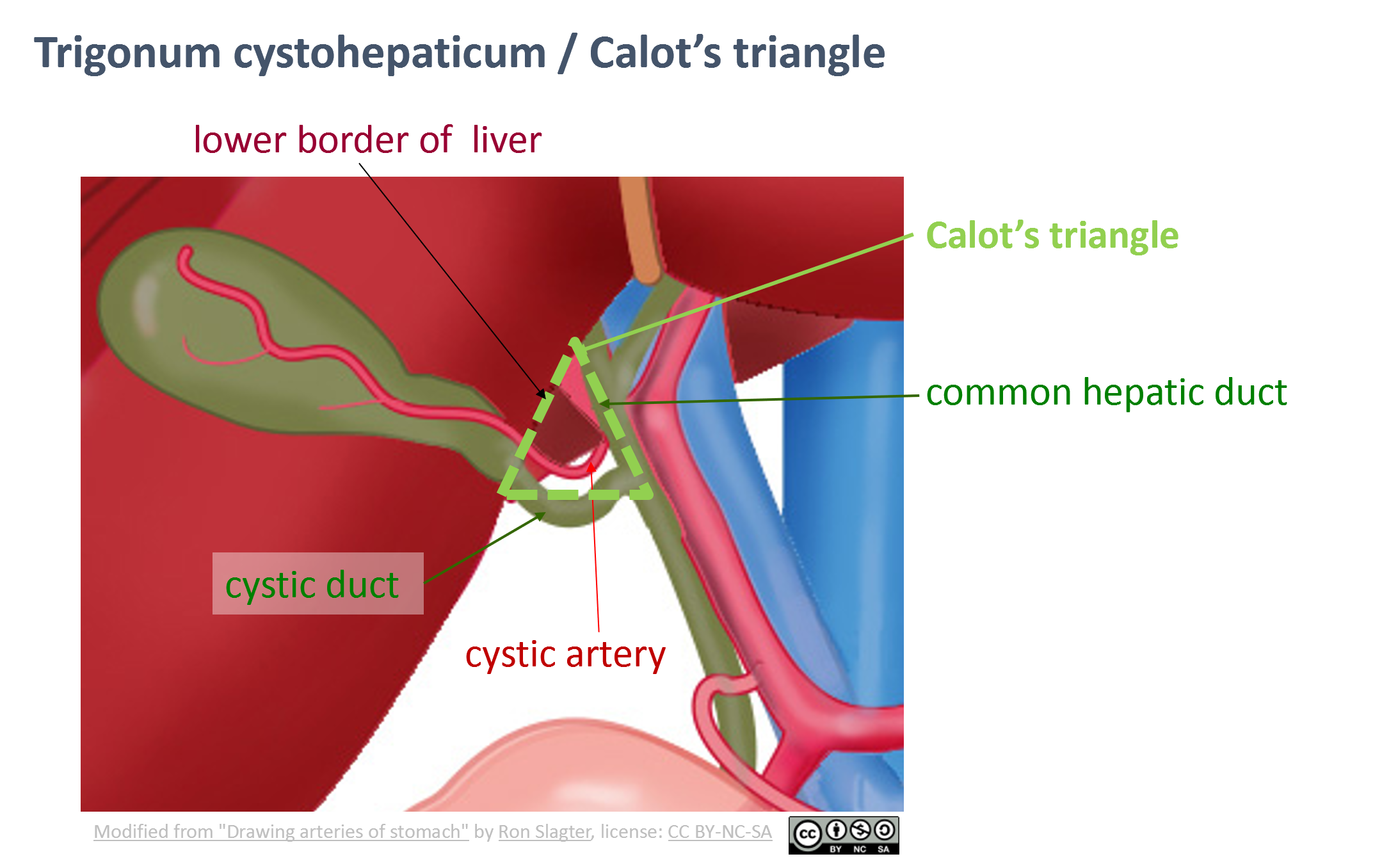
Calot’s Triangle (Hepatocystic Triangle)
One of the most important anatomical landmarks in cholecystectomy surgical anatomy is Calot’s Triangle (also known as the hepatocystic triangle).
Boundaries
- Medial: Common hepatic duct
- Inferior: Cystic duct
- Superior: Inferior surface of the liver
Contents
- Cystic artery
- Lymph node (Node of Lund)
- Variable arterial branches
Meticulous dissection in this triangle is critical for identifying and ligating the cystic duct and cystic artery safely.
The Critical View of Safety (CVS)
Modern laparoscopic surgery emphasizes achieving the Critical View of Safety (CVS) before dividing any structures.
To achieve CVS:
- Clear the hepatocystic triangle of fat and fibrous tissue
- Separate the lower one-third of the gallbladder from the liver bed
- Ensure only two structures (cystic duct and cystic artery) enter the gallbladder
This technique significantly reduces bile duct injuries and is a cornerstone of safe cholecystectomy surgical anatomy.
Arterial Supply in Cholecystectomy Surgical Anatomy
The primary blood supply to the gallbladder is the cystic artery, typically arising from the right hepatic artery.
Key Points:
- Usually found within Calot’s triangle
- May have anatomical variations
- Can present as multiple branches
Anatomical variations occur in up to 25% of patients, making careful dissection essential.
Venous Drainage
Venous drainage of the gallbladder occurs through:
- Small veins draining directly into the liver
- Cystic veins draining into the portal venous system
Bleeding during dissection of the gallbladder bed often originates from small hepatic veins.
Lymphatic Drainage
Lymphatic drainage flows to:
- Cystic lymph node (Node of Lund)
- Hepatic lymph nodes
- Celiac lymph nodes
Understanding lymphatic pathways is particularly important in cases of suspected gallbladder malignancy.
Nerve Supply
The gallbladder receives autonomic innervation from:
- Sympathetic fibers (celiac plexus)
- Parasympathetic fibers (vagus nerve)
Pain from gallbladder pathology is often referred to the right shoulder due to diaphragmatic irritation via the phrenic nerve.
Anatomical Variations in Cholecystectomy Surgical Anatomy
Variations are common and increase surgical complexity.
Cystic Duct Variations
- Short cystic duct
- Long parallel course alongside CBD
- Low insertion into CBD
- High insertion near hepatic ducts
Arterial Variations
- Double cystic artery
- Cystic artery arising from aberrant hepatic artery
Bile Duct Variations
- Accessory bile ducts (ducts of Luschka)
- Aberrant right hepatic duct
Failure to recognize variations is a leading cause of bile duct injury.
Liver Bed Anatomy
The gallbladder is attached to the liver by connective tissue and small vascular channels.
During cholecystectomy:
- Dissection proceeds from infundibulum toward fundus
- Care must be taken to avoid bleeding
- Ducts of Luschka may cause postoperative bile leaks
Understanding liver bed anatomy is essential for preventing complications.
Laparoscopic Perspective of Cholecystectomy Surgical Anatomy
Laparoscopic surgery changes depth perception and orientation.
Important considerations include:
- Camera angle visualization
- Retraction of gallbladder to expose Calot’s triangle
- Maintaining correct anatomical planes
Proper exposure and traction-countertraction techniques enhance anatomical clarity.
Common Complications Related to Surgical Anatomy
Poor understanding of cholecystectomy surgical anatomy may result in:
- Common bile duct injury
- Hemorrhage
- Bile leak
- Retained ductal stones
Bile duct injury remains one of the most serious complications, often requiring reconstructive surgery.
Safe Dissection Techniques
To minimize risk:
- Avoid blind clipping
- Identify structures clearly before division
- Convert to open surgery if anatomy is unclear
- Consider intraoperative cholangiography when necessary
Safety should always take priority over speed.
Inflammation and Distorted Anatomy
In acute cholecystitis, inflammation can distort anatomy:
- Edema thickens tissue planes
- Adhesions obscure Calot’s triangle
- Cystic duct may be difficult to identify
In such cases, alternative techniques like subtotal cholecystectomy may be considered.
Role of Intraoperative Imaging
Intraoperative cholangiography (IOC) can help:
- Identify bile duct anatomy
- Detect stones in CBD
- Prevent bile duct injury
It is especially useful in uncertain anatomical situations.
Teaching and Training in Cholecystectomy Surgical Anatomy
Surgical education emphasizes:
- Cadaveric dissection
- Simulation training
- 3D anatomical models
- Video-based learning
Thorough anatomical training reduces complication rates.
Importance of Preoperative Imaging
Ultrasound, MRCP, or CT scans help evaluate:
- Gallstones
- Bile duct dilation
- Anatomical anomalies
Preoperative planning improves intraoperative decision-making.
Conclusion
Cholecystectomy surgical anatomy forms the foundation of safe gallbladder removal. Mastery of biliary structures, vascular supply, anatomical variations, and critical safety principles is essential for preventing complications.
From identifying Calot’s triangle to achieving the critical view of safety, every step depends on precise anatomical knowledge. As laparoscopic techniques continue to evolve, understanding three-dimensional surgical anatomy remains more important than ever.